
Tooth replacement with dental implants is considered the standard of care for replacing the natural tooth system in the contemporary practice of dentistry. Their success rates have been well documented in the dental literature over the last half century. Advances in surgical and prosthetic techniques have allowed for more conservative surgical approaches to pave the way to achieve more predictable wound healing and less soft tissue changes: critical issues in the aesthetic zone. Metal-free implant designs are proving to be an additional component to achieving natural soft-tissue emergence profiles and eliminate the potential for soft-tissue complications that titanium implants and abutments present, especially in compromised soft-tissue volume and thickness.
The following article will demonstrate the immediate restoration procedure in the aesthetic zone with multiple implant placement and provisionalisation utilising one-piece metal-free implants. The use of dental implants for tooth replacement procedures has become commonplace in the treatment planning process for dentists and dental specialists.1, 2 During the last twenty years, variations in the conventional, multistep process of implant reconstruction have begun to demonstrate the benefits of immediate restoration, especially in the aesthetic zone.3–8 These benefits include minimally invasive protocols, shortened treatment times, preservation of soft-tissue contours and emergence profiles, and delivery of a stable, aesthetic, provisional restorations (instead of a removable temporary) that can begin the process of tissue sculpting and forming the final emergence profile.9 –11 Ensuring the appropriate volume and quality of the peri-implant soft tissues, especially in the aesthetic zone, is paramount not only for the peri-implant environment and long-term maintenance of bone levels but also for long-term aesthetic results that can be achieved.8 –11 The incorporation of metal-free dental implant designs into, not only the holistic dental practice, but also for routine daily use in the contemporary general and specialty practice has increased over the last several years.12–16 The benefits of zirconia dental implants, which include a high level of biocompatibility, reductions in the formation of biofilm and its resultant decrease in bacterial plaque accumulation, heightened level of fracture toughness, and the reduction in bone loss levels long-term in the implant bone crest, and soft tissue attachment areas, are a distinct alternative to titanium for an implantable implant material.17–21
Conventional titanium two-piece implant designs have been extensively studied over the last 25 years in regard to the connection between the implant/abutment complex, and the micro-gap issue that exists and can be an introductory point for bacterial invasion into the peri-implant environment, becoming an initiation point for crestal bone loss and peri-mucositis and peri-implantitis formation.22–28 One-piece titanium implant designs theoretically reduced the micro-gap issue, but design limitations can increase aesthetic complications and accelerate peri-implant and bone and soft-tissue loss. Two-piece zirconia implant designs reduce the micro-gap issue as a result of the decrease in biofilm formation and the reduction in soft-tissue inflammation, an important pre-curser to peri-mucositis and peri-implantitis.29 One-piece zirconia implant designs offer additional benefits in that elimination of the micro-gap space between the zirconia implant and abutment being non-existent and reduction of biofilm formation virtually eliminated. In various zirconia implant one-piece designs, the ability to not only prepare the abutment portion of the implant, but also the collar and/or implant portion of the zirconia fixture allow for superior characteristics for an implant to replace the natural tooth system.30–33 The following case report will demonstrate the use of one-piece zirconia implants to replace the natural tooth system in multiple sites in the aesthetic zone.
Case report
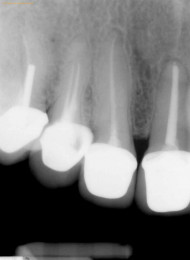
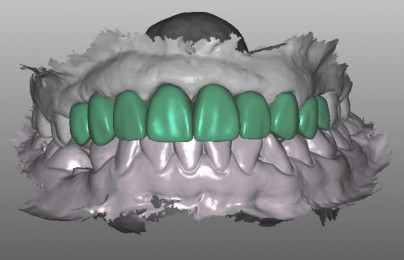
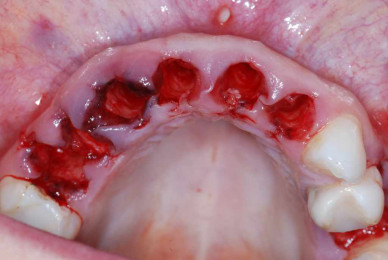
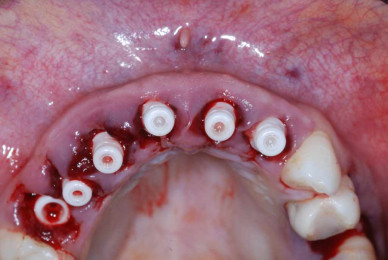
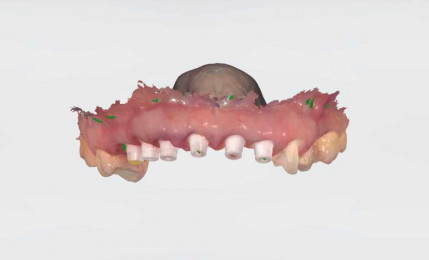
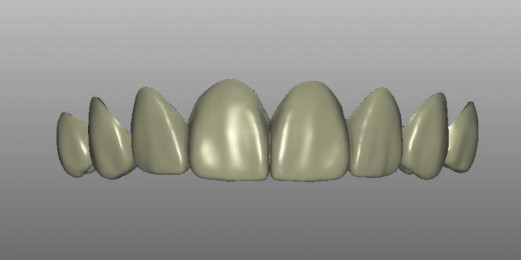
A forty-one-year-old non-smoking female presented for treatment of gingival erythema, missing teeth, failing root canals and wanting aesthetic enhancement of the maxillary anterior aesthetic zone (Figs. 1 & 2). The patient also complained of a dull ache in the maxillary anterior, and an overall feeling of malaise. Figures 3 and 4 show the pre-operative digital periapical views. Multiple root canal treated teeth were present with restorations invading the biologic width environment in the areas of the maxillary right second premolar to the maxillary left lateral incisor. Additionally, the maxillary left second premolar required replacement. Figure 5 demonstrates ill-fitting and mis-proportioned full coverage metal-based restorations with multiple biologic width impingements. After consultation with the patient, review of medical and dental histories, and an aesthetic interview with the patient, the treatment plan consisted of the removal of all maxillary teeth with root canals and poor fitting metal base restorations, and the placement of one-piece zirconia implants in the areas of maxillary right first premolar to maxillary left central incisor, veneers at the maxillary left canine and first premolar and two-piece zirconia implants at the maxillary second premolars. Following a digital workflow, pre-operative 3D scanning of the maxillary arch was accomplished (Fig. 6) and sent to an aesthetic laboratory technician to design the ideal 3D plan to address the aesthetic concerns of the patient (Fig. 7). This 3D plan becomes the digital blueprint to design the aesthetic provisionals and serve as a precursor to the final aesthetic planned restorations. After administration of pre-operative antibiotics, an appropriate local anaesthetic in the maxillary arch was given, and the teeth slated for extraction were removed by an atraumatic tooth removal process, preserving the gingival soft tissue emergence profiles (Figs. 8 & 9). Please note the tissue hyperplasia and inflammation in the maxillary right area. Care is taken to not disrupt the natural tissue emergence profiles, facial gingival margin and remaining alveolar contours to perform a minimally invasive implant placement and bone regeneration procedure. Following site preparation, the extraction sites were replaced with one-piece implants (SDS Swiss Dental Solutions) and two-piece implants (SDS Swiss Dental Solutions) in the second premolar sites (Figs. 10 & 11). All implants achieved an initial torque measurement of 50 Ncm.







Following minimally invasive implant placement, autologous platelet-rich fibrin, prepared from a blood draw pre-surgically, was used to rehydrate a fully resorbable ceramic graft material (Osseolive, curasan) and the A-PRF/Osseolive complex placed peri-implant in the void between the implant surface and the residual buccal plate gap space remaining post-extraction and implant placement. Digital scanning post-insertion of the implants and communication with the original 3D smile design allows for printing off of the provisional shell (Fig. 12). The provisional shell is then retrofitted, and margins verified. Cementation of the provisional is then completed with ETC temporary cement dual cure (Parkell). Excess cement is removed, and bite evaluation/adjustment completed. The immediate postoperative clinical view can be seen in Figure 13. Two months post-implant placement the patient was appointed for 3D scanning and secondary provisional fabrication. Figure 14 demonstrates the clinical appearance of the zirconia implants and resultant soft tissue contours obtained from the initial immediate restoration procedure. Figure 15 shows the 3D scanning view which is then blended with the initial smile design (Fig. 16) and the new provisional, with updated contours to ensure natural emergence profiles, papillary contours and interproximal tissues is printed, and seated again with provisional cement. Figure 17 shows the aesthetic provisional with final soft tissue profiles 10 days post-secondary provisional seating. Please note the aesthetic soft tissue contours created and maintained to support natural aesthetics in the final restorations. Figure 18 shows the 3-month post-insertion digital peri-apical radiograph and Figure 19 is the facial view of the final provisional restorations prior to initiation of the final all-ceramic restorations.






Conclusion
Tooth replacement in the aesthetic zone has become a highly predictable procedure utilising immediate restoration protocols that have been well documented in the dental literature over the last 15 years. Minimally invasive protocols to preserve natural soft tissue contours present after tooth removal have been shown to cause less soft-tissue complications in the final restoration, especially in the aesthetic zone. Incorporating one-piece zirconia implants into the immediate restoration protocol offers additional benefits over titanium as a dental implant option; improved soft tissue response, virtually non-existent biofilm formation, micro-gap elimination between the implant/abutment complex and heightened aesthetics are normally achieved in the final all-ceramic restorations. Additionally, with one-piece zirconia implant designs, especially with a zirconia composition that allows the clinician to prepare the abutment, collar and base aspect of the implant itself, and additional level of flexibility is present in the instance that additional preparation is necessary for the correction of compromised bone and soft-tissue contours, or to correct angulation issues present due to malpositioning of the implant complex. As the success rates of zirconia implants continue to be positive in the dental literature, their position as a common option for tooth replacement will continue to rise and gain popularity in the dental implant field.
A list of references can be accessed at https://qr.oemus.com/8975
Image credit: Dr Paul S. Petrungaro