
Currently, the majority of ceramic implants used are one-piece implant systems, which, however, have some limitations and disadvantages.1, 2 One-piece implants cannot always be inserted in the optimal orientation and require angulation correction to enable prosthetic restoration. In addition, one-piece implants are subjected to soft tissue and chewing forces immediately after insertion. These reasons motivated the development and manufacture of two-piece ceramic implants. Several two-piece ceramic implants are already available on the market, but only limited clinical evidence is available for these systems. Currently, a large proportion of two-piece ceramic implants have a bonded implant–abutment connection. While bonded zirconia abutments have promising clinical results,3, 4 there is uncertainty about the long-term stability of the adhesive bond between the implant and abutment and the biological effects of adhesive residues in the area of the gingival sulcus.
Concerning two-piece screw-retained ceramic implants, in vitro studies showed higher fracture rates compared to two-piece titanium implants or one-piece zirconia implants.5 The weak location for increased fracture susceptibility is the area directly around the abutment screw. Further studies are needed to indicate the ideal connection design for two-piece screw-retained zirconia implants. Additionally, the exact influence of different cementation and crown materials on the loading capacity of two-piece screw-retained zirconia implants is still uncertain.1, 6 Further preclinical evidence for the prosthetic restoration of two-piece screw-retained zirconia implants is required to provide practical recommendations for clinical use. The aim of this in vitro study was to investigate the survival rate and the relationship between prosthetic complications and the type of crown fixation after dynamic loading of CAD/CAM-fabricated anterior monolithic lithium disilicate crowns mounted on two-piece screw-retained zirconia implants.
Materials and methods
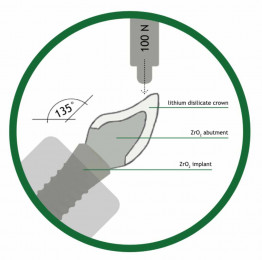
Twenty two-piece screw-retained zirconia implants (4 mm in diameter and 12 mm in length; CERALOG Hexalobe®, CAMLOG) were each fitted with an individualised zirconia abutment (Figs. 1 & 2, Figs. 5–7) and embedded in acrylic resin (Fig. 10). The abutment aspect was optically scanned, and a standardised upper left incisor-shaped ceramic crown was designed (Figs. 11 & 12). Twenty lithium disilicate crowns were milled, sintered and mounted on the implants (Figs. 3 & 4, Figs. 8 & 9) either with an adhesive resin composite cement (Multilink Automix®, Ivoclar Vivadent; Group A, n = 10) or with a resin modified glass ionomer cement (FujiCEM 2®, GC; Group B, n = 10). All samples underwent thermomechanical loading at an angle of 135° (Fig. 13) to simulate an aging of five years (TCML; TC: 5 °C and 55 °C, 3,000 cycles, 2 min/cycle; ML: 100 N, 1,2 x 106 cycles). The evaluation of prosthetic complications was compared with the Mann-Whitney-U-Test. The significance level was set to α = 0.05.









Results
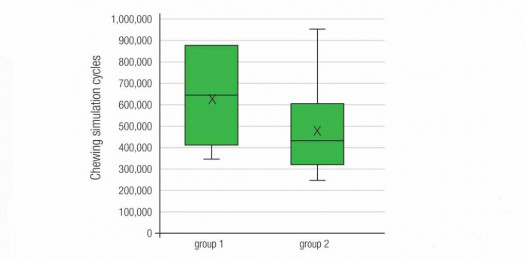
The 5-year survival rate of both groups (n = 20) after artificial ageing was 95 % (Fig. 13). One abutment of Group B fractured after 1,123,200 cycles. All specimens in both groups had grinding facets. In group A grinding facets had an overall mean appearance of 639,360 ± 200,106 cycles with no significant difference (p > 0.05) to group B with 483,840 ± 208,800 cycles (Fig. 14). None of the samples showed cracks, fractures or decementations of the crown.



Conclusions and clinical implications
Of course, long-term, clinical, randomised trials are one of the best ways to generate reliable data. But it is necessary to implement preclinical study designs that simulate clinical conditions before clinical trials are conducted. Thermomechanical loading of implants, abutments and crowns offers a suitable method for this. Within the limitations of this preclinical trial it can be concluded that CAD/CAM-fabricated anterior monolithic lithium disilicate crowns mounted on two-piece screw-retained zirconia implants should provide sufficient resistance at least up to five years of intra-oral forces. Regarding prosthetic complications, there was no statistical difference between using an adhesive resin composite compared to a resin-modified glass ionomer cement for crown cementation. It can be assumed that different manufacturing methods or design properties of two-piece screw-retained ceramic implants lead to variable fracture behaviour under load. A generalisation for two-piece screw-retained ceramic implants does not yet seem to be possible. Further studies are needed.
A list of references can be accessed at https://qr.oemus.com/8033
Image credit: Drs Manuel Reinisch, Elisabeth Steyer, Martin Koller; Profs. Norbert Jakse, Michael Payer, Karl Glockner