
Introduction
Advancements made in the dental zirconia industry have given rise to new and alternative treatment options for implantology. When compared with other ceramic oxides, zirconia exhibits outstanding biochemical properties. Since its introduction to dentistry, it has been utilised as a material suitable for fixed dental prosthesis, ceramic crowns, metal-free implant abutments and prosthetic frameworks. Zirconia is highly suitable for dental implants owing to its tooth-like colour, structure, material properties and biological response. Additionally, human studies indicate minimised adhesion of bacteria to zirconia compared with titanium. Zirconia also exhibits fewer inflammatory cells within the peri-implant soft tissue. A recently conducted systematic review showed a 95 per cent survival rate of one- and two-piece zirconia implants after one year of successful functioning.1 According to this article, the marginal bone loss and survival values of one- and two-piece zirconia implants after a year is acceptable. Also, it must be highlighted that there is a lack of data specifying the performance of zirconia implants in long-term studies, and thus, it has become increasingly important to further research these implants and to obtain more data. In the following, a clinical case is depicted in which a maxillary premolar is replaced using a one-piece ceramic implant following a digital workflow from treatment planning to prosthetic rehabilitation.
Initial situation
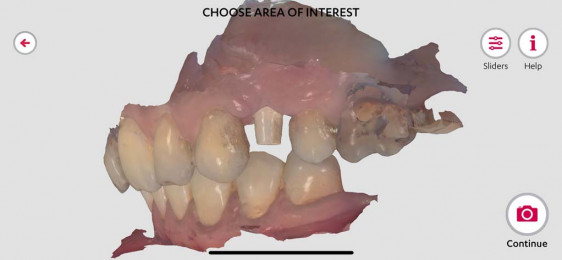
A 44-year-old patient attended the scheduled dental maintenance appointment complaining of a fractured tooth (Fig. 1), which had been treated endodontically and restored with a crown five years prior. The patient was a non-smoker and had an otherwise unremarkable medical history. Clinical assessments revealed little pain during percussion. A periapical radiograph confirmed the clinical findings and revealed the fracture line to be at the cervical margin of tooth #24. A horizontal root fracture was diagnosed and the patient agreed to his tooth being replaced with a metal-free ceramic implant.

Digital planning
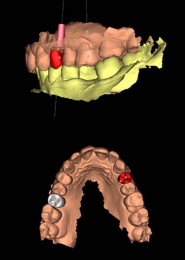
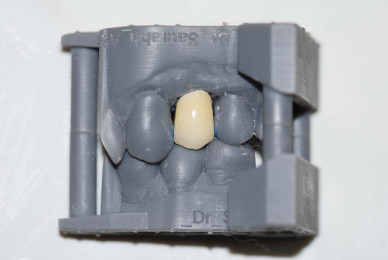
A digital design software programme was used for designing the surgical guide and for implant planning. CBCT scans were combined with an open-format surface in the planning software for gaining a comprehensive clinical insight (Fig. 2). The benefits of prosthetic-based implant planning for achieving optimal function and aesthetics were considered while accounting for the current clinical situation, including bone density, soft-tissue type and anatomy, and projected prosthesis. A customised surgical guide was designed based on the planned position of the implant (Fig. 3). The provisional restoration was digitally designed and fabricated by the laboratory technician for immediate restoration.

Surgical procedure
On the day of surgery, a pre-surgical dose of 600 mg of ibuprofen and 750 mg of amoxicillin was administered to the patient. Atraumatic extraction was carried out to remove the root tip (Fig. 4). The manufacturer’s instructions were followed for placing the conventional surgical guide and preparing the implant bed. Implant indicators were used for preparing and maintaining an accurate vertical position for placing the monotype zirconia implant. A ZiBone zirconia implant (COHO Biomedical Technology) with a diameter of 4.0 mm, a body length of 11.5 mm and an abutment height of 4.0 mm was surgically placed by means of guided surgery without the need for a flap (Fig. 6). After being placed at a torque of 35 Ncm, the implant showed good primary stability. The minor buccal bone defect was corrected using bone cement (Augma Biomaterials) to enhance the vestibular ridge contour and to give the crown a natural appearance (Fig. 7). A horizontal mattress silk suture was placed for closure (Fig. 8). Also, the acrylic provisional restoration fabricated prior to the surgery using the implant design software was inserted immediately after the surgical procedure (Figs. 9–13). A chlorhexidine mouthrinse, an anti-inflammatory and antibiotics were prescribed. The suture was removed seven days after the implant placement.









Prosthetic phase
The osseointegration was successful and it was planned to restore the implant using a zirconia crown after four months. The abutment portion was prepared using Magic Touch burs (Strauss & Co.), and an intraoral optical scan (TRIOS 3 Wireless, 3Shape) was taken of the abutment portion of the monobloc zirconia implant (Figs. 14 & 15). Self-adhesive resin cement (3M ESPE) was used after cleaning and air-drying the zirconia surfaces. Excess cement was removed carefully using dental floss after cementation of the final crown. Control and maintenance appointments were scheduled six months and one year after placement of the implant (Figs. 16 & 17). The implant crown was still functional and no technical complications were observed at either appointment. The soft tissue surrounding the implant with respect to site #24 was quite healthy. A periapical radiograph was taken at the one-year follow-up. Bone re-modelling around the implant was normal and the level of bone surrounding the border had fully stabilised. The patient was satisfied with the treatment outcome, in terms of both aesthetics and function.




Conclusion
No technical or biological complications were recorded after one year of implant functioning. Thus, the use of a zirconia implant in this case turned out to be a suitable alternative to a titanium implant. The soft tissue surrounding the implant was stable and exhibited outstanding biocompatibility. The vertical implant position is an important factor for success of such implants, as the soft-tissue collar of the implant needs to be apically positioned at a depth that allows for soft-tissue apposition and attachment up to the restorative platform. For such a one-piece implant, the process of restoration requires cementation, which bears the risk of excess cement being retained subgingivally, leading to complications ranging from bone loss to implant failure.
A list of references can be accessed at https://qr.oemus.com/7070
Image credit: Drs Saurabh Gupta, Sammy Noumbissi